Last updated: July 15, 2026 | By Richard Hale
TENS (Transcutaneous Electrical Nerve Stimulation) machines send low-voltage electrical current through electrode pads placed on the skin, stimulating nerves in a way that can block or reduce pain signals. They are among the most widely used home pain management devices. The evidence for TENS is real but condition-specific — it works meaningfully for some types of joint and nerve pain, and has little effect on others.
This content is for educational purposes only and is not medical advice. TENS devices are contraindicated in some individuals — see the safety section before using. Do not use TENS if you have a pacemaker or cardiac defibrillator without clearance from your cardiologist.
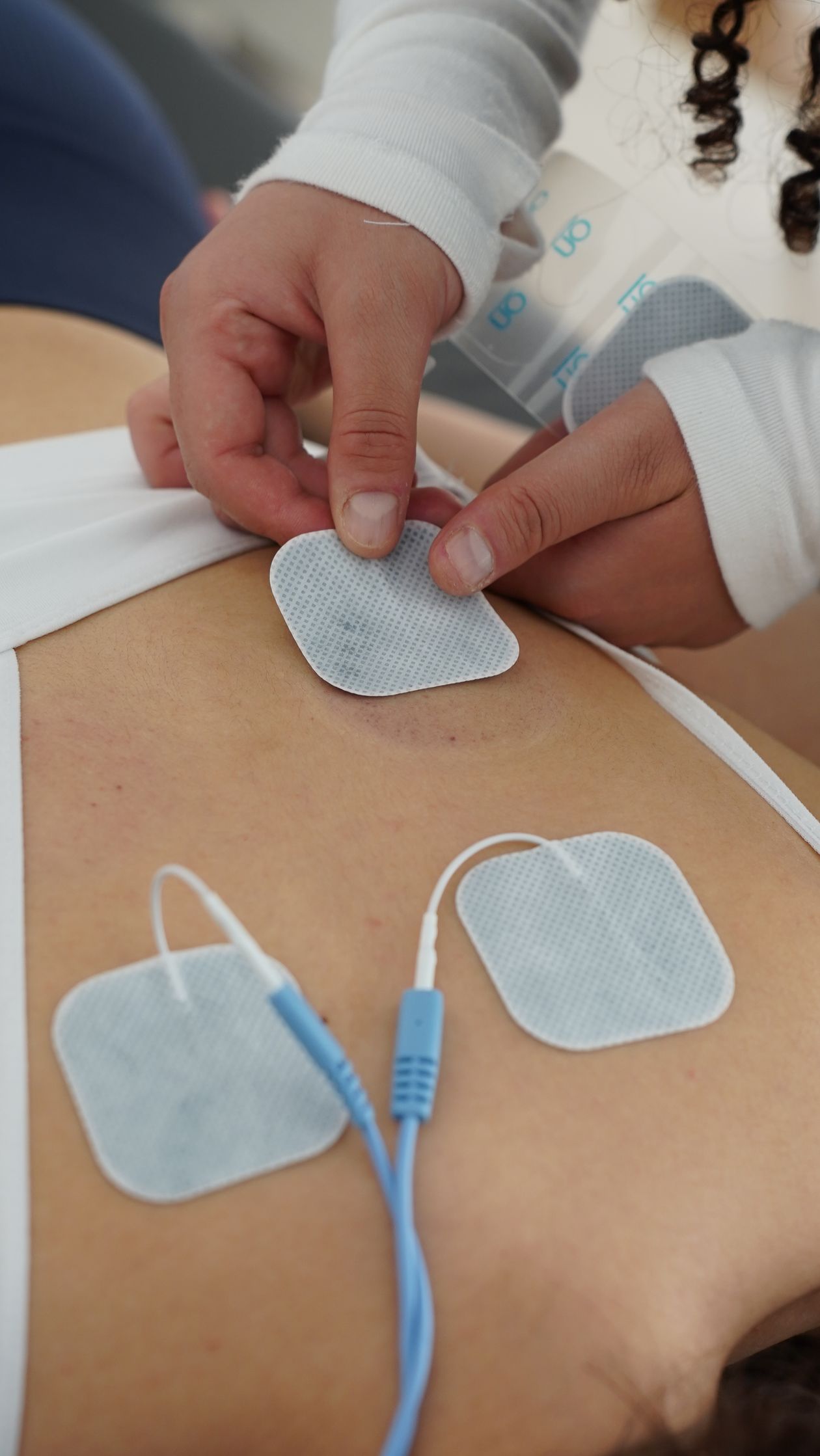
Table of Contents
- How TENS Works
- Evidence by Condition
- How to Use a TENS Unit Correctly
- Types of TENS: Conventional vs. Acupuncture-Like
- Safety and Contraindications
- Choosing a TENS Unit
- Frequently Asked Questions
How TENS Works
TENS produces pain relief through two primary mechanisms, which operate at different electrical parameters:
Gate control theory (high-frequency TENS): the spinal cord contains a “gate” mechanism that determines which pain signals pass up to the brain. Stimulating large-diameter sensory nerve fibers (A-beta fibers) with high-frequency electrical current activates interneurons that close this gate — blocking smaller-diameter pain-carrying fibers (A-delta and C fibers) from transmitting their signals upward. This is the same mechanism that explains why rubbing a bumped elbow temporarily reduces the pain. High-frequency TENS (80-150 Hz) produces pain relief within minutes that typically lasts during and shortly after the session.
Endorphin release (low-frequency TENS): low-frequency TENS (1-10 Hz) at higher intensities stimulates A-delta fibers, triggering the release of endogenous opioids (endorphins, enkephalins) in the spinal cord and brainstem. This mechanism has a slower onset (20-30 minutes) but produces longer-lasting pain relief, sometimes persisting hours after the session ends. It is blocked by opioid antagonists like naloxone, confirming the endorphin mechanism.
Evidence by Condition
Knee osteoarthritis: the best-studied joint condition for TENS. A 2015 Cochrane review of 18 RCTs found that TENS produced significant short-term pain reduction in knee OA, with effect sizes comparable to NSAIDs during the treatment period. The evidence is strongest for symptom management during activity and for morning stiffness. A practical limitation: the pain relief does not persist long after treatment cessation, so TENS is best understood as a daily or frequent pain management tool rather than a curative treatment.
Chronic low back pain: mixed evidence. Multiple reviews find TENS superior to sham TENS for pain relief, but effect sizes vary considerably across studies. The American College of Physicians clinical guidelines include TENS as a recommended non-pharmacological option for chronic low back pain. For acute low back pain, evidence is weaker.
Neuropathic pain: TENS has reasonable evidence for conditions with a neuropathic (nerve pain) component — diabetic peripheral neuropathy, post-herpetic neuralgia, and chemotherapy-induced neuropathy. The gate control mechanism is particularly relevant for nerve pain conditions.
Rheumatoid arthritis: TENS is generally not recommended during active inflammatory flares — electrical stimulation can increase local blood flow, potentially worsening acute inflammation. It may provide pain relief in stable periods between flares but should not be applied over actively inflamed joints.
Fibromyalgia: moderate evidence. Several RCTs show TENS reduces movement-evoked pain in fibromyalgia. The University of Iowa has conducted notable research showing 4 weeks of TENS use improved pain, fatigue, and physical function in fibromyalgia patients.
How to Use a TENS Unit Correctly
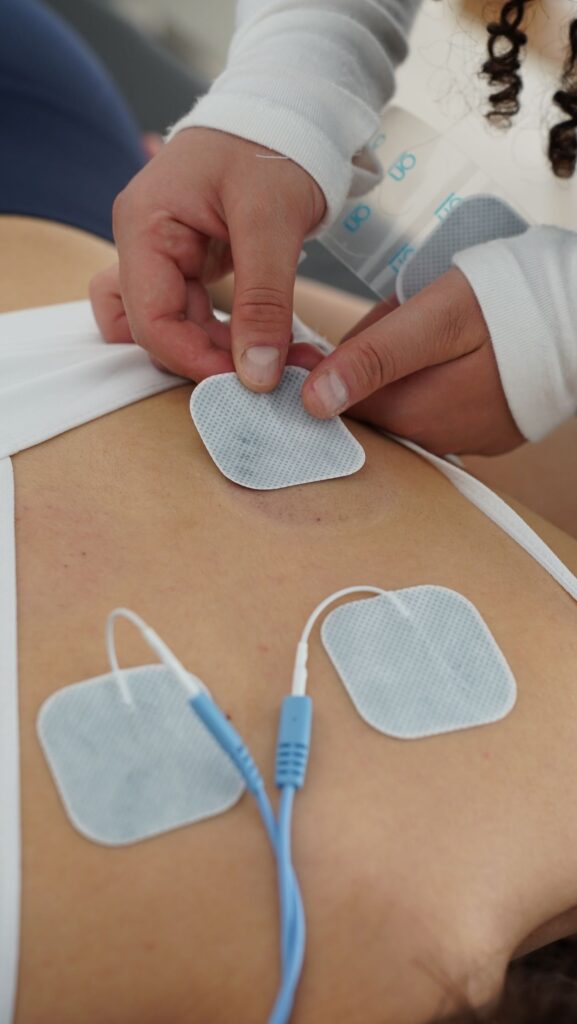
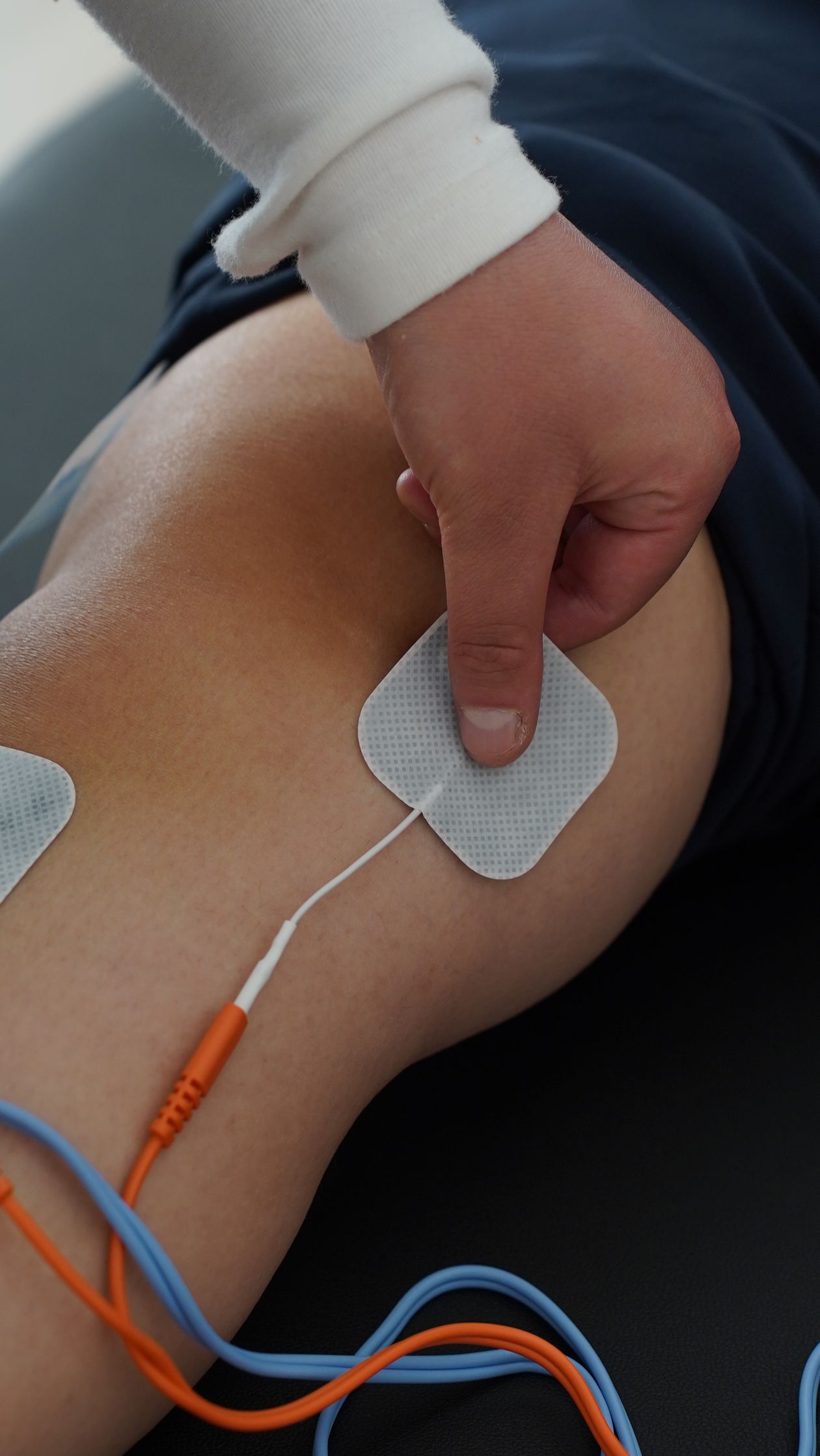
Electrode placement: place electrodes directly around the painful area — on either side of the joint, or surrounding the pain location. For knee pain, this means medial and lateral placement around the joint line. For lower back, on either side of the lumbar spine. Do not place electrodes directly over bone prominences or joints — on the surrounding soft tissue. The electrical current should pass through the painful area between the electrode pads.
Intensity: start at the lowest intensity and increase gradually until you feel a strong but comfortable tingling or buzzing sensation. For conventional (high-frequency) TENS, you should feel the sensation without muscle twitching. For acupuncture-like (low-frequency) TENS, muscle twitches are expected and intentional. Never increase to a painful intensity — if it hurts, reduce it. More intensity is not more effective for conventional TENS.
Session duration: 20-45 minutes per session is typical and sufficient. Longer sessions do not proportionally increase benefit and may cause skin irritation from the electrode pads. Starting with 20-minute sessions and assessing response before extending is a reasonable approach.
Frequency: daily use is appropriate for chronic pain management. For acute pain episodes, multiple daily sessions (2-3 times/day) can be used. Some devices have auto-shut-off after 60 minutes as a safety feature — this is appropriate.
Types of TENS: Conventional vs. Acupuncture-Like
Conventional TENS (high-frequency): 80-150 Hz frequency, lower amplitude, produces tingling sensation without muscle contraction. Onset of pain relief is rapid (within minutes). Most consumer TENS devices default to this mode. Best for: general pain management, OA, low back pain.
Acupuncture-like TENS (low-frequency): 1-10 Hz frequency, higher amplitude, produces rhythmic muscle twitches. Onset slower (20-30 minutes) but duration of relief after session is longer. Targets endorphin release. Best for: chronic neuropathic pain, fibromyalgia, and when conventional TENS provides insufficient relief duration.
Burst TENS: delivers bursts of high-frequency impulses at a low repetition rate — combines elements of both mechanisms. Some people who do not respond well to either conventional or AL-TENS respond to burst mode. Less studied but used clinically.
Safety and Contraindications
Absolute contraindications:
- Cardiac pacemaker or implantable defibrillator: TENS can interfere with the device’s sensing function. Do not use without specific clearance from your cardiologist.
- Do not place electrodes on the chest or in the transthoracic position (current crossing the heart).
- Do not place electrodes on the anterior neck or over the carotid sinuses (can cause blood pressure drops or laryngeal spasm).
- Pregnancy: do not use over the abdomen or lower back.
- Epilepsy: avoid stimulation over the head or neck.
- Do not use over open wounds, infected skin, or areas with impaired sensation.

Choosing a TENS Unit
Consumer TENS devices range from under $40 to over $200. The key features to look for are adjustable frequency and intensity controls, at least 4 channels (to allow multiple electrode placements simultaneously), a timer, and replaceable electrode pads. Whether a device has FDA clearance as a 510(k) device indicates it met basic safety and manufacturing standards for medical devices — this is the relevant quality marker for US consumers, not total price.
Brands with strong clinical and consumer track records include Omron, iReliev, and TensCare. Many physiotherapy clinics use devices in the same therapeutic range as quality consumer units. The primary difference in clinical settings is that a physiotherapist guides electrode placement and intensity for your specific condition — the technology itself is similar.
Frequently Asked Questions
Can I use TENS every day?
Yes. Daily use is appropriate for chronic pain management conditions like knee OA, chronic low back pain, and neuropathic pain. Multiple sessions per day are also acceptable for acute flares, as TENS has no systemic side effects (unlike daily NSAIDs). The main practical limitation is electrode pad longevity — pads typically last 20-30 sessions before their adhesion degrades and they need replacement. Cleaning the skin area before application extends pad life significantly.
Is TENS the same as EMS (electrical muscle stimulation)?
No. TENS is designed to stimulate sensory nerves for pain relief, using parameters (frequency, intensity) calibrated to produce sensation without overwhelming muscle contraction. EMS (electrical muscle stimulation) uses higher intensities and different parameters specifically to produce forceful muscle contractions for muscle strengthening or rehabilitation. Some devices combine both functions in different modes. Using a TENS device at EMS-level intensities is uncomfortable and not intended — check which mode you are using before adjusting intensity.
About the author: Richard Hale is an independent health writer focused on mobility, joint health, and active aging research. He is not a licensed medical professional. All content on VitalMove40 is for educational purposes only and is not a substitute for advice from a qualified healthcare provider.





